December 2025
Inside This Issue
 Accreditation 360:
Accreditation 360:
Happy Holidays! In reviewing this month issue of Perspectives, the good news is there are no new and unexpected additional requirements to scramble around to implement. Much of the issue is focused on JC’s new Accreditation 360 redesign, which in another month will be the format surveyors and organizations will be using. Hopefully our readers have been studying and preparing for the new format.
NPG Briefs:

We did note one article discussing “NPG Briefs” that was informative. JC has posted to its website, simple 2-page briefs discussing the standards in the National Performance Goals chapter. There are links provided in Perspectives to help find these briefing documents.
We were a little surprised in reading the document titled “NPG #1, Right Patient, Right Care.” The discussion on the standards at first seemed to blur multiple requirements together, but then we realized it was discussing all the different standards starting with NPG.01.01.01 – NPG.01.06.03, not just NPG.01.01.01.
This review also caused us to re-examine the 629 page survey process guide, which we believe will likely be the most informative document for readers to rely on as it contains both the standards and their elements of performance as well as techniques surveyors will use to evaluate compliance with those elements of performance. The techniques include interviews with selected staff, document reviews including policies and procedures, medical records, meeting minutes, logs, PI data, as well as direct observation of care processes.
These “NPG Briefs” appear to be high level summaries that may be more useful for discussion with media or public audiences who want to know summary information about patient safety standards. For preparation purposes we would recommend using the survey process guide.

New Standards Webinars:
Perspectives also has an article about the webinars JC produced to help explain the new standards format in different chapters. If you have not viewed these as yet, we would suggest doing so. These were informative and detailed. Links are provided in the Perspectives article for 8 chapters.
 Signs, Placards, Labels and Legends:
Signs, Placards, Labels and Legends:
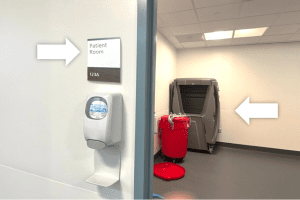
The December issue of EC News has a very detailed article discussing the problems that organizations can have with required signage or labeling of piped medical gases, medical gas cylinders, electrical panels, eyewash stations, fire door assemblies, fire extinguishers, and exit signage.
Piped medical gas shut off valves must be labeled with the name or chemical symbol of the gas, plus identify the rooms affected by the shut off valve and include a warning not to open or close the valve except in an emergency. We see labels, either inside the plastic cover or externally mounted on the wall can fall off over time. Sometimes rooms are repurposed and the room identifier no longer makes sense. For example, what used to be called Exam Room 1 may now be a storeroom or an office, or vice versa.
![]() Cylinders of medical gases also have complex labeling requirements. Central storage of oxygen and/or medical air cylinders must be labeled “Medical Gases: NO Smoking or Open Flame.” Storerooms containing other gases must have labels stating: “Positive Pressure Gases: NO Smoking or Open Flame. Room May Have Insufficient Oxygen. Open Door and Allow Room to Ventilate Before Entering.”
Cylinders of medical gases also have complex labeling requirements. Central storage of oxygen and/or medical air cylinders must be labeled “Medical Gases: NO Smoking or Open Flame.” Storerooms containing other gases must have labels stating: “Positive Pressure Gases: NO Smoking or Open Flame. Room May Have Insufficient Oxygen. Open Door and Allow Room to Ventilate Before Entering.”
Central stores of oxidizing gases including oxygen and nitrous oxide must be labeled “CAUTION: OXIDIZING GASES STORED WITHIN. NO SMOKING.”
Electrical panel labels can be similarly problematic. Each breaker must identify what it controls, and spare breakers should never be in the ON position. If any breaker is on, it must identify what part of the area it controls.
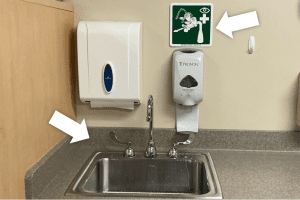
Eyewash stations and drench showers must be labeled to identify to staff where they need to go in the event of a hazardous chemical eye splash. A well-lit, visible sign should direct staff to the eyewash and that eyewash should be readily available within 10-seconds (typically interpreted as no more than 55-feet) of where corrosive chemicals are being used. Also, a door is also considered an obstruction. If the hazard is non-corrosive, one (1) door can be present if it opens in the same direction of travel as the person requiring the use of the flushing station.
Fire doors, door frames and any windows in the fire door must be labeled to document the fire protection rating, certified as tested, include the manufacturer’s name, the certifying agency and fire test designation. Labels may not the painted over rendering this required content illegible. Labels can also fall off over time, so you want to verify your labels are intact and legible during your annual inspection process.
Fire extinguishers that are contained within a cabinet or where visibility is otherwise blocked must be labeled to identify that a fire extinguisher is present. The special K-type fire extinguisher commonly stored in the kitchen must include a placard reminding staff that the overhead fire suppression system must first be activated before using the K-type extinguisher.
Exit signage is required above every exit door, and along exit routes where the path![]() may not be clear. Externally illuminated exit signs must have lettering that is 6-inches in height. Other exit signs must be 4-inches in height. NO EXIT signs must be used wherever an incorrect pathway might be mistaken for an exit. NO EXIT labels must be 2-inches high for the word “NO”, and the word “EXIT” must be 1-inch high, labeled below the word NO.
may not be clear. Externally illuminated exit signs must have lettering that is 6-inches in height. Other exit signs must be 4-inches in height. NO EXIT signs must be used wherever an incorrect pathway might be mistaken for an exit. NO EXIT labels must be 2-inches high for the word “NO”, and the word “EXIT” must be 1-inch high, labeled below the word NO.
Focusing on medical gas shut off valve labeling, electrical panel breaker labeling, medical gas cylinder storage labeling, eyewash station labels/access, fire door assemblies, fire extinguisher labels, exit signage, and no exit labels would be a really good internal tracer checklist of high risk, commonly cited issues.

Very importantly, the EC News article also reminds that the detailed requirements currently in the elements of performance disappears next year under the new standards PE.04.01.01 and PE.03.01.01 which simply points us to compliance with NFPA requirements.
Another interesting aspect to consider for 2026 is that each of these issues were quite frequently scored noncompliant independently. In 2026 all labeling deficiencies that are noncompliant with an NFPA required labeling expectation will be scored against just two standards, PE.03.01.01 and PE.04.01.01 and the noncompliance rate on each is likely to be very high.
New Facilities Guidelines:
 If you have any construction or renovations planned for the coming year, you will want to look at the EC News article entitled: “Healthcare Design Tips.” They advise us that currently JC expects approved construction projects to use the 2022 FGI Guidelines. The authors provide a heads up that in spring 2026, revised FGI Guidelines are anticipated for hospitals, outpatient facilities and residential care settings.
If you have any construction or renovations planned for the coming year, you will want to look at the EC News article entitled: “Healthcare Design Tips.” They advise us that currently JC expects approved construction projects to use the 2022 FGI Guidelines. The authors provide a heads up that in spring 2026, revised FGI Guidelines are anticipated for hospitals, outpatient facilities and residential care settings.
Imaging Safety:
The December issue of EC News has an article summarizing where JC has moved their imaging safety standards for 2026. Those JC standards that equate to CMS  requirements are located under PE.05.01.01 and those that JC believes exceed CMS requirements are placed under four (4) NPG standards, NPG.13.01.01, 13.02.01, 13.03 and 13.04.01. In addition, JC has provided a link to another of JCR’s checklist tools for imaging and equipment safety. You will want to share this tool with your radiology team for them to assess compliance and meet to discuss their findings.
requirements are located under PE.05.01.01 and those that JC believes exceed CMS requirements are placed under four (4) NPG standards, NPG.13.01.01, 13.02.01, 13.03 and 13.04.01. In addition, JC has provided a link to another of JCR’s checklist tools for imaging and equipment safety. You will want to share this tool with your radiology team for them to assess compliance and meet to discuss their findings.
 DNV:
DNV:
DNV has posted a link to register for their 2026 Healthcare Symposium planned for the Kalahari Resort in the Wisconsin Dells. You can register for the event and when more content is posted regarding the agenda by visiting their Attend the 2026 DNV Healthcare Symposium events page.
CIHQ:
CIHQ has information posted this month about two (2) webinars that will be taking place in December. Both webinars have a fee assigned for those organizations that don’t use either their accreditation or consulting services.

- The first is Compliance Expectations for Translation and Interpreter Services. This will be held on December 18th at 2PM Eastern Standard Time. The link to register is available at this webinar’s Webinar Center page.
- The second webinar is Preparing for the 2026 TJC Standards Changes for the Physical Environment. This will be held on December 17th. The link to register is available at this webinar’s Webinar Center page.
ACHC:

Join health care leaders March 2–4, 2026, in Amelia Island, FL for ACHCU Academy 2026, a multi-day conference focused on strengthening accreditation, compliance, and quality across post-acute and home care settings. The event offers expert-led sessions, practical strategies, and valuable networking for professionals in home health, hospice, ambulatory care, pharmacy, renal dialysis, and more. Registration is now open.
Update on USP Chapter 797 Compliance:

We have not seen anything recently in Joint Commission’s publications about what they are citing relative to USP Chapter 797, however a publication on November 4th from Pharmacy Practice News, Results Are in From New NABP Verified Pharmacy Program Inspections, did highlight findings from surveys being conducted by the National Association of Boards of Pharmacy, NABP.
One of the findings seen in 11% of their surveys was a failure to formally identify a designated person in charge and responsible for oversight of sterile compounding activities. As a reminder there should be an appointment letter in a person’s HR file documenting that they are the DP or designated person.
The article also noted that 22% of cleanroom suites had environmental surfaces that were not cleanable due to defects such as cracks in flooring or unsealed surfaces. Another noticeable problem is that 23% of vendor certification reports were missing required content such as the number of personnel present during testing.
Two new expectations from the revised Chapter 797 were requirements for master formulation records (“how to” recipes) and compounding records (documenting the compounding). These were absent for master formulations 21% and compounding records 14% of the time.
 QSO-26-02 Noncompliance During Shutdown:
QSO-26-02 Noncompliance During Shutdown:
The Federal government is now open again and CMS has issued one new QSO on November 24th. This is QSO-26-02 and it affects all provider types, but most of the guidance is directed toward state agencies, explaining how to document federal noncompliance if applicable that was noted during a “state licensure only” survey during the shutdown. This guidance is important to the states because they can cost allocate the survey to CMS.
The memo consists of 14 frequently asked questions that have come from the states to CMS. Questions 7 and 12 specifically address findings that may now be issued against CMS standards that would have been scored deficient during a state standards-only survey conducted during the federal shutdown.
CONSULTANT CORNER
As we reach the end of the year, we’re reminded how much dedication and thoughtful effort is poured into strengthening care across healthcare settings. From teams refining their daily processes to leaders advancing safer practices, your commitment continues to shape better outcomes for patients and communities.
Whether through progress in survey readiness, safer environments of care, or more reliable clinical processes, the work you’ve contributed this year has created a stronger foundation for what lies ahead.
Your efforts elevate the quality, safety, and experience of care every single day, and as the year turns, we hope the months ahead bring renewed energy, clarity, and success.
In the spirit of the season, we’re sharing a complimentary gap analysis tool for the new OB requirements to support your work as you prepare for the year ahead. Please use it as-is or personalize it to your team’s needs.
Click on your gift to download a copy.

Thank You!
Julia Finken, RN, BSN, MBA, CPHQ, CLSSMBB
Julia.finken@hbsinc.com
Jen Cowel, RN, MHSA
jencowel@pattonhc.com
Yvonne Rockwood, MBA, MHA, CPHQ
yvonnerockwood@hbsinc.com