August 2025
Inside This Issue
Accreditation 360:
This month’s edition of Perspectives discusses The Joint Commission’s new approach to accreditation that they are calling Accreditation 360. They are very enthusiastic and optimistic about their new approach. One of the enhancements mentioned is that the standards are going to be posted on their website and available to the public starting in July. We checked as we were drafting this newsletter, and we don’t see the standards posted yet, however the pre-publication standards are. It will be interesting to see if they follow through on this plan as the sale of manuals was always a large revenue producer that we assume they would not want to diminish.
 A second change discussed is to “shift the focus from observation of structure and process to outcome measures, creating a next generation certification program for maternity care, hip and knee procedures, spine procedures and cardiovascular procedures.” That too will be interesting as meaningful performance measurement has long been viewed as an attractive, potential alternative to routine onsite survey presence.
A second change discussed is to “shift the focus from observation of structure and process to outcome measures, creating a next generation certification program for maternity care, hip and knee procedures, spine procedures and cardiovascular procedures.” That too will be interesting as meaningful performance measurement has long been viewed as an attractive, potential alternative to routine onsite survey presence.
The third change is what they call Survey Analysis For Evaluating Strengths, or SAFEST. Perspectives indicates that this will become a “database of leading practices where surveyors can access an organization’s performance strengths for industry wide collaborative learning.” The term “surveyors can access” seemed unusual as accredited organizations have in the past recommended access to such a database. This also will be interesting to see how it evolves.
New Obstetrical Services Requirements:

The new draft 2026 manuals were posted last month and now we have new obstetrical services standards as a result of a CMS final rule, CMS-1809-FC, posted back in November 2024. This final rule contains the obstetrical requirements, but they are buried within a larger outpatient prospective payment and ambulatory surgical rule that is hundreds of pages long.
We sometimes find these larger rules confusing as they include discussion about comments submitted to CMS relative to proposed rules and sorting out what is approved and what is not is a challenge. We would suggest instead going to the eCFR site available. At this link you can search for just the five (5) very specific changes to the hospital CoPs that relate to the new standards developed by TJC. These specific CMS references are detailed in the Perspectives article and in the draft standards posted to The Joint Commission’s prepublication page.
New Standards: Effective Immediately:
 Joint Commission has three (3) standards with new content that are effective immediately. These are referenced with their 2025 and 2026 standards numbers. HR.01.05.03 which next year becomes HR.11.03.01 has four (4) new elements of performance relative to education and training of staff for provision of emergency services. Each EP has very specific CMS standards references that you can look up on the eCFR site for additional details. In summary these four (4) elements of performance require training annually on protocols and provisions implemented for emergency services, identification by the governing body of who must take this education, demonstration that staff have acquired new knowledge, and refinement of education based on analysis by QAPI.
Joint Commission has three (3) standards with new content that are effective immediately. These are referenced with their 2025 and 2026 standards numbers. HR.01.05.03 which next year becomes HR.11.03.01 has four (4) new elements of performance relative to education and training of staff for provision of emergency services. Each EP has very specific CMS standards references that you can look up on the eCFR site for additional details. In summary these four (4) elements of performance require training annually on protocols and provisions implemented for emergency services, identification by the governing body of who must take this education, demonstration that staff have acquired new knowledge, and refinement of education based on analysis by QAPI.
The second standard that is effective immediately is LD.04.03.01, which becomes LD.13.03.01 next year. Here there are three (3) new elements of performance which in summary require that your provision of emergency services and protocols be in accordance with your complexity and scope of services, your protocols are consistent with evidence-based guidelines and last, your equipment, supplies, and emergency medications be readily available to meet the needs of your patients.
Each of these first two standards and their EPs tie back to CFR.482.55. If you study the eCFR for §482.55 you will pick up some additional details such as a requirement to have the emergency services supervised by a qualified member of the medical staff and each emergency services treatment area must have a nurse call system for each patient.
The third and final new requirement effective immediately is PC.04.01.03 which becomes PC.14.01.01 next year and it has only one new element of performance. This EP requires policies and procedures for transfer of patients to an appropriate level of care, including another hospital as needed to meet the needs of each patient. In addition, there should be annual training of staff regarding these policies and procedures for transfer of patients. The CoP reference, §482.43(c) states in the eCFR that: “The hospital must use findings from its QAPI program to inform staff training needs and any additions, revisions, or updates to training topics on an ongoing basis.”
New Standards: Effective Jan 1, 2026:
 Then effective January 1, 2026, there are four (4) standards with five (5) new or modified elements of performance. These all tie back to the CoP reference §482.59 and surprisingly don’t look as if they should require a significant implementation effort.
Then effective January 1, 2026, there are four (4) standards with five (5) new or modified elements of performance. These all tie back to the CoP reference §482.59 and surprisingly don’t look as if they should require a significant implementation effort.
The first 2026 standard, LD.13.01.07, EP 4 requires that a hospital that provides obstetrical services to place all labor and delivery rooms and suites under the supervision of an experienced registered nurse, certified nurse midwife, nurse practitioner, physician assistant or a Doctor of Medicine or Osteopathy.
The second 2026 standard is LD.13.03.01, has three (3) EPs, the first of which is EP 1. This just adds obstetrical services to a long list of services routinely provided by hospitals; however, provision of obstetrical services remains a choice. EP 23 requires that if you provide obstetrical services, they be consistent with the needs and resources of the hospital. EP 24 then requires that if you provide obstetrical services that the hospital have adequate provisions and protocols, consistent with nationally recognized, evidence-based guidelines for obstetrical emergencies, complications, immediate post-delivery care and other patient health and safety events as identified as part of the QAPI program. There are two deemed status notes with this EP, the first of which ties back to a CoP reference at §482.21 for QAPI, and the second note identifies a CoP reference §482.59(b)(1) for equipment needed.
The third standard, MS.17.02.01 states that if obstetrical services are provided, obstetrical privileges are delineated for all practitioners providing obstetrical care in accordance with the competencies of each practitioner. This seems like a rather routine expectation rather than an onerous new requirement.
The fourth and last new standard, PC.12.01.05, EP 2 describes expected equipment including a call in system, cardiac monitor, and fetal doppler or monitor.
Although the timeline to implementation is nonexistent for some of these requirements, for the most part, these are likely things that already exist. The requirements for documented training (HR.11.03.01, EP 2) of all staff identified by the governing body (HR.,11.03.01, EP 3) to be in need of training is likely to be the most difficult or time consuming new requirement to implement. The requirement for written policies and procedures for transferring patients to other inpatient facilities for an appropriate level of care (PC.14.01.01, EP 15) may require some fine tuning, and in addition, details about such policies should be a part of the previously mentioned training.
Sentinel Event Data:
 In April we had mentioned in our newsletter that Perspectives had referenced the 2024 annual review of sentinel event data, but at that time the link to the data was not working. The August issue of Perspectives again says the data is now available and this time the link did work. The total volume of reports continues to grow, and they present the ten (10) most frequently reported types of sentinel events.
In April we had mentioned in our newsletter that Perspectives had referenced the 2024 annual review of sentinel event data, but at that time the link to the data was not working. The August issue of Perspectives again says the data is now available and this time the link did work. The total volume of reports continues to grow, and they present the ten (10) most frequently reported types of sentinel events.
By a large margin, falls is the most frequently reported sentinel event, amounting to almost half of all reported sentinel events, and with 51 of those events resulting in patient death. Details are also provided about the wrong surgery events with 68% being wrong site, 12% wrong patient, 11% wrong procedure and 9% wrong implant. We would encourage readers to take a look at the data as there are always learning opportunities from the mistakes of others, that might enable strengthening your safeguards.
2026 Standards Re-write and Workplace Violence:
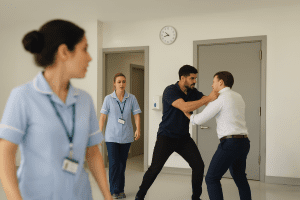
EC News has an article about the new 2026 standards manual and the consolidation of their workplace violence standards into one chapter under NPG, or National Performance Goals. The consolidation of these requirements we believe makes analysis easier than the scatter method. As consultants we often retained the original prepublication standards because the printout contained all the standards associated with a single concept in a concise format, rather than multiple chapters. In the past, issues such as resuscitation, workplace violence, imaging device QC checks and others appeared in multiple chapters from EC to HR, to PI, depending on the nature of the requirement. Having issues like this reconsolidated may be helpful. If you’re still just beginning your analysis of this 2026 standards manual, you might want to start with the NPG chapter.
Tips for Preventing Surgical Fires:
 The August issue of EC News has a nice review of techniques and tips to prevent surgical fires that we would encourage you to share with your operating room staff. They may find this content particularly valuable for developing training materials.
The August issue of EC News has a nice review of techniques and tips to prevent surgical fires that we would encourage you to share with your operating room staff. They may find this content particularly valuable for developing training materials.
The authors identify that 90-100 surgical fires occur each year and then discuss many prevention or mitigation strategies from Fire Risk Assessment, training, fire drills, preoperative preparation, safe use of germicides, equipment and energy source safety, equipment handling, ignition source control, oxygen and anesthesia safety, team communication and situational awareness and risk awareness and reporting.
Generator Testing:
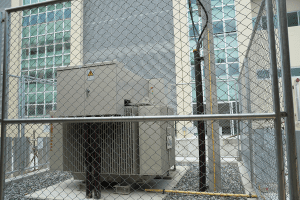 The August issue of EC News has a Q&A article on generator testing that appears to be a helpful refresher on the detailed requirements of generator testing. We often see one or more of the details on how a generator should be tested that are missing, either identified by our consultants or by TJC. That caused us to look to see how this complex issue is addressed in the 2026 manual.
The August issue of EC News has a Q&A article on generator testing that appears to be a helpful refresher on the detailed requirements of generator testing. We often see one or more of the details on how a generator should be tested that are missing, either identified by our consultants or by TJC. That caused us to look to see how this complex issue is addressed in the 2026 manual.
The 2025 standard is EC.02.05.07 and we noted that the detailed elements of performance that identify how to test the generator have been deleted for 2026. The crosswalk that identifies where 2025 requirements went indicates this content is in the new 626-page Survey Process Guide. What remains in the 2026 standards is the essence of this complex requirement, PE.04.01.03, EP 3, is to test the emergency power source in accordance with NFPA 99-2012. It will be interesting to see if the new simplified manual leads to higher compliance or a higher rate of findings. While it still exists, this Q&A might be helpful to use in verifying you have all the requirements for generator testing embedded in your existing processes.
![]()
DNV: HealthHub Newsletter Updates:
A new DNVHealthHub July 2025 Edition Newsletter posted to their Supply Chain and Product Assurance LinkedIn on July 29th. It highlights their latest updates and offerings in healthcare accreditation, including their integration of ISO 9001 quality standards, details on the upcoming Healthcare Symposium, stroke center certification, infection prevention training, and current promotions and events.
 ACHC: Inpatient Prospective Payment Systems (IPPS):
ACHC: Inpatient Prospective Payment Systems (IPPS):
ACHC recently published a Regulatory Update, Medicare Program; Hospital Inpatient Prospective Payment Systems for Acute Care Hospitals (IPPS) and the Long-Term Care Hospital Prospective Payment System and Policy Changes, on August 3. You will find this update to be applicable to both acute and critical care hospitals and will go into effect on October 1, 2025.
![]() CIHQ: Dialysis Webinar with NDAC:
CIHQ: Dialysis Webinar with NDAC:
CIHQ is holding a free webinar, CIHQ Partner Webinar Series – NDAC, in partnership with the National Dialysis Accreditation Commission (NDAC) on August 12 at 12pm CST. As dialysis is always such a focus of attention by accreditors or CMS, you may be interested to register for this program.
 Covid PHE Memo Revision:
Covid PHE Memo Revision:
On July 30th, CMS issued three (3) QSO memos, the first of which is a revision QSO memo, QSO-25-23-ALL, that modifies QSO-23-13, dated May 1, 2023, that discussed guidance to all provider types during the Covid public health emergency (PHE). As the PHE has already ended, there really is not much new information contained in this revision.
There is a reminder for nursing home providers that the focused infection control surveys are no longer part of the standard survey process, but that complaints about infection control issues will still be conducted through complaint investigations. There is also guidance to the hospital industry that had participated in the acute hospital at home program. Although the blanket waivers have expired, this program had been continued as a result of Congressional actions. The QSO provides a link to a AHCAH page on the CMS website. When you go to that site it states that without additional Congressional action, the acute hospital at home program will end on September 30th.
Nursing Home IC Survey Process Memo Expired:
The second QSO issued on July 30th, QSO-23-10-NH, causes an earlier memo, QSO 23-10 directed to the nursing home industry, to expire. That memo had established the focused infection control survey process for nursing homes, which has now ended.
 Nursing Home “Late Adopters” Program Expired:
Nursing Home “Late Adopters” Program Expired:
The third memo issued on July 30th, 19-07-NH, causes an even earlier QSO 19-07 memo directed to the nursing home industry to also expire. The title of that memo had been “Enhanced Oversight and Enforcement of Non-Improving Late Adopters.” The focus of that program had been to reduce unnecessary psychotropic drug use in nursing homes. The expiration memo directs readers to the State Operations Manual, Appendix PP for nursing homes, tag F605. While the “late adopters” focused program may be ended, tag F605 still indicates that CMS has an intense focus on psychotropic drug use to verify that they are not being used as chemical restraints of convenience.
CONSULTANT CORNER
I wanted to personally inform you about some exciting leadership changes at HBS, Patton, and Barrins! As part of my long-term plan and a step toward my eventual retirement, I’ve been working diligently to ensure that Patton is in the right hands to continue serving you with the excellence you’ve come to expect from us.
As many of you know, Patton Healthcare Consulting, along with Barrins & Associates, integrated with HBS over three years ago. This has proven to be a smooth and successful partnership, enhancing the quality and breadth of services we provide to clients. With that said, it is my pleasure to announce that I will be handing over the executive leadership of HBS Accreditation and Regulatory Compliance to Julia Finken. I’ve had the privilege of working closely with Julia for nearly three years, and I have seen firsthand her dedication, passion, and strategic thinking. Julia has played a pivotal role in driving our vision forward.
While Julia assumes leadership, I will continue to manage the day-to-day operations at Patton, ensuring continued success and the ongoing support of our valued clients.
Additionally, we are excited to welcome Yvonne Rockwood to our team! Yvonne will manage the day-to-day operations of Barrins, as well as our behavioral health, home care, and post-acute as well as select hospital clients. Yvonne has been a trusted consultant with us and brings over 30 years of leadership experience, including her work with The Joint Commission. She also served as a former COO at a Northern California hospital and as an administrator for home care and post-acute services. Yvonne’s wealth of expertise will be invaluable as we continue to enhance and expand our offerings.
We are deeply appreciative of your continued trust and partnership. With Julia, Yvonne and I at the helm, we are committed to maintaining the highest level of service and collaboration, and I look forward to the continued success of our work together.
Please feel free to reach out if you have any questions or would like to discuss further.
Best,
Jen
Thank You!
Jennifer Cowel, RN MHSA
JenCowel@PattonHC.com
Kurt Patton, MS RPh
Kurt@PattonHC.com
Julia Finken, RN, BSN, MBA, CPHQ
julia.finken@hbsinc.com
John Rosing, MHA
JohnRosing@PattonHC.com