February 2025
Inside This Issue

IC & Antibiotic Stewardship Resource Center:
This month’s edition of Perspectives has news and updates, but nothing to make you stop and change your plans for the month. There is one article about a new infection prevention and antibiotic stewardship resource center on their website that was interesting. We went to the site and began exploring the search criteria and you can scroll through all the content, but it is of course time consuming if trying to focus on a particular issue. Fortunately, there is also a search feature that allows you to search for resources in a much more focused way.
You will want to share the site information with your infection prevention and antibiotic stewardship leaders, who may like to examine the available content.
Wall and Ceiling Penetrations:
This month’s Consistent Interpretation column focuses on penetrations and the requirements of LS.02.01.10, EP 14. The scoring of this EP is huge with 45% of last year’s hospital surveys being scored noncompliant. Penetrations have also been a persistent issue on survey throughout all our careers.
It should not be this difficult, but unfortunately there are many different staff, contractors, and vendors who may be up above your suspended ceilings drilling holes, running pipes or cables who don’t understand the requirements. These contractors may also be accustomed to working with a wide variety of sealants, many of which are not actually approved fire stops.
The core requirement is that the hole or gap around a pipe or cable must be sealed with an approved fire protectant sealant. The article identifies 3 potential approval bodies including ASTM, UL, or NFPA that can approve the sealant. Most importantly, an expanding foam sealant is not the right type of fire protection because it is combustible.
As consultants, we like to think of this as a management design issue, such as, how can we eliminate the chance or error in this process. There are two immediate potential errors, one being not sealing the penetration at all and second not sealing the penetration with the appropriate type of sealant.
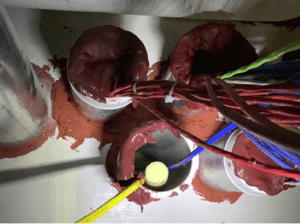 There is also a delayed, third chance of error and that is using a sealant that is a different color from all the other surrounding sealants. It may be an approved sealant, and you may have verified it carried the mark of approval from ASTM, UL or NFPA, however 5 years from now when a surveyor asks to see the specifications for that unusual color sealant, you won’t be able to find the information needed.
There is also a delayed, third chance of error and that is using a sealant that is a different color from all the other surrounding sealants. It may be an approved sealant, and you may have verified it carried the mark of approval from ASTM, UL or NFPA, however 5 years from now when a surveyor asks to see the specifications for that unusual color sealant, you won’t be able to find the information needed.
We would also suggest two recommendations to foolproof this process. First is a permitting an inspection process whenever anyone goes up above your ceiling to perform work. During the permitting process you would educate the contractor about your requirements which would of course detail specifications for fire sealants in penetrations. In addition, you can take this opportunity to educate them about your infection prevention expectations and not draping or connecting any cables or piping to existing sprinkler pipes.
At the conclusion of the contractor project, you would then want to inspect their work to verify compliance with your expectations so that you are protected from future survey surprises. In addition, you could consider financial incentives and/or penalties for noncompliance with your requirements.
New Survey Report Format:
This month’s lead article discusses the new survey report format and the terminology for specific elements of performance that have been added to the SAFER Matrix. As this was discussed last month in Perspectives and in this newsletter, we won’t belabor the issue, but we can add that we have seen an example of the new survey report and the modifications to the SAFER Matrix do provide a nice summary glimpse at what the detailed report includes. This should be great for summarizing data for administrative leaders.
 Bariatric Mobility and Facility Design:
Bariatric Mobility and Facility Design:
The February issue of EC News has an interesting article on designing facilities to accommodate bariatric patients. There are some potentially helpful web links to resources in the article including one to a Veterans Administration Bariatric Safe Patient Handling and Mobility Workbook.
From a design perspective, the article discusses some of the patient devices that are being manufactured for larger patients such as larger beds, however these larger beds may not be able to pass through existing room doors. The authors suggest a split door with two different size leaves, one of which can usually be fixed, but opened when needed to accommodate larger equipment passing through the door.
The authors also advise about routine equipment such as grab bars, toilets and scales, which may be called upon to handle more weight than usual, pointing out that there is specialized equipment available that can handle higher weights.
Security Risk Advice:
 The February issue of EC News has a very useful article on tips for managing security risks. The authors suggest:
The February issue of EC News has a very useful article on tips for managing security risks. The authors suggest:
- Include a broad array of clinical leaders, IT, HR, EM, and facilities staff, not just your safety and security experts in your security risk assessment. In addition, be sure to include representatives from high-risk departments such as the ED and Behavioral Health and consider including local law enforcement to help advise about community risks.
- When designing a reporting and tracking system for security incidents, be sure to include those related to workplace violence, along with space to describe the interventions used and the relative success of those interventions for potential lessons learned.
- When issuing temporary identification to visitors, contractors, consultants or others be sure to include names and destinations where the visitor is authorized to be, and if possible, include photo identification on the temporary ID.
- When considering or installing security cameras, panic buttons or other devices, evaluate the inspection, testing and maintenance requirements for the devices planned.
- If installing weapons detection systems, be sure not to adversely affect egress from the building and seek guidance from the authority having jurisdiction in your area, relative to egress.
- If considering weapons detection systems, factor in the technology used and its potential effects on patients with implanted medical devices.
- If considering arming security officers, or the use of K-9s, conduct a risk assessment and detail policies on training, handling and potential use of weapons.
- If designing construction or renovation of the emergency department, consider adding an adjacent behavioral health crisis unit. EC News also advises that there are now FGI design guidelines for such units.
- Lastly, don’t overdo it to the extent that access to the facility and in particular the emergency department is hindered.
Basic Building Information (BBI):
 This month’s Q+A column discusses the Basic Building Information (BBI) requirements on your Joint Commission extranet. The BBI provides detailed information for surveyors and in particular the life safety code specialists so they know what they need to see and areas to focus on during survey. Each site must have its own form included on the BBI, but a site with multiple connected buildings can be prepared on one form. The authors explain that a stand-alone business occupancy does not need to be included, however if that business occupancy is contained in a building that is mostly an ambulatory or healthcare occupancy it must be included on the BBI.
This month’s Q+A column discusses the Basic Building Information (BBI) requirements on your Joint Commission extranet. The BBI provides detailed information for surveyors and in particular the life safety code specialists so they know what they need to see and areas to focus on during survey. Each site must have its own form included on the BBI, but a site with multiple connected buildings can be prepared on one form. The authors explain that a stand-alone business occupancy does not need to be included, however if that business occupancy is contained in a building that is mostly an ambulatory or healthcare occupancy it must be included on the BBI.
The article details 21 different pieces of information that the BBI requires for each building and that the surveyors will review that information prior to arrival. As you never want to surprise your surveyors with unanticipated sites they must visit, or missing details about a site that would cause them to need additional time to review that site, it is advisable to carefully review your BBI and keep it up to date as conditions change.
Environmental Disasters:
 TJC issued Sentinel Event Alert Issue 69 in November on Environmental Disasters and Preparing to Evacuate or Shelter in Place. At that time the southeastern portion of our nation was starting to recover from Hurricane Milton, and since publication we have now seen the wildfires in California.
TJC issued Sentinel Event Alert Issue 69 in November on Environmental Disasters and Preparing to Evacuate or Shelter in Place. At that time the southeastern portion of our nation was starting to recover from Hurricane Milton, and since publication we have now seen the wildfires in California.
The SE Alert starts by describing how the standards help guide planning for disasters with the HVA analyzing your unique risks, the EOP describing what we will do, and the COOP describing who will lead us if not all our administrative leaders are present.
The Alert provides six (6) recommendations for consideration:
- Revisit and update your emergency plans: There is much that can be learned from recent disasters, and we will likely see additional publications describing how organizations in these recent disaster areas coped, and what worked along with what did not work adequately. But the advice here would be to revisit, reanalyze current EM planning with the knowledge of how likely such disasters are in your area.
- Establish and build collaborative relationships: If your organization is severely impacted by the disaster, you may need support to evacuate and transfer patients to other care providers. Where are you going to go and who is going to help with transportation? Identifying such partner relationships ahead of time will make things go more smoothly if ever needed.
- Develop a resilient communications infrastructure: The severity of the disaster could knock out the traditional communication methods. Landlines and cell phones could be out, and you want to have plans for alternatives. They discuss satellite phones, walkie talkies and even ham radio as potential options.
- Plan how to meet essential needs and provide care to staff and patients: Whether you shelter in place or evacuate, you will still need to provide care, and have access to supplies including food, water, linens, medications, IV fluids and other supplies. You will also need the staff to provide care, and these staff will need to sleep, shower, and eat as well.
- Plan and practice how to evacuate or shelter in place: Evacuation practice will provide insight on how long it takes, how many people need to be involved, what routes to take down to the ground level and thus how long it will take and how quickly you need to start the evacuation in order to accomplish it successfully. Such planning should also consider how to manage ventilator dependent patients, pediatric patients, those with limited English proficiency and other special needs patients.
- Recovery: As we see in magnitude of the disasters in the southeast and in California, recovery may take a long time. Planning for continuing services may not involve returning to your home base in just a few days.
 ACHC: ACHCU Academy 2025:
ACHC: ACHCU Academy 2025:
The ACHCU is conducting their ACHCU Academy seminar at the Fairmont Hotel in Dallas, TX on March 3-5 and the agenda looks like it will cover a wide array of useful subjects. In looking at the agenda it appears that it would be informative for its clinical content regardless of which accrediting body you use.
 ACHC: Becker’s Hospital Review Webinar:
ACHC: Becker’s Hospital Review Webinar:
Three (3) speakers from ACHC and two (2) others from health systems will be presenting in a free webinar on accreditation options and experience. The Myth-busting: Learn the Truth about Hospital Accreditation Options webinar will be available on demand from Becker’s Hospital Review.
 ACHC: Most Frequent Findings:
ACHC: Most Frequent Findings:
The ACHC semiannual publication called Surveyor did a summary of the most frequent findings in the Surveyor, Volume 2024, No.2. These findings of course link to specific ACHC standards, but as the different accreditors all link to the same CMS CoP requirements and important clinical issues, this information may be helpful to all readers.
 DNV: Infection Prevention Podcast:
DNV: Infection Prevention Podcast:
DNV posted a new podcast to Spotify on January 9th called, Risks in Infection Prevention. These podcasts are convenient in that they can be listened to on your computer or in the car while driving to work. The speakers converse about some of the more common IP issues which arise on DNV surveys. The podcast can be located on Spotify by searching DNV or using the link above.

Laboratory SOM Update:
On January 17, CMS issued QSO 25-13 which updated their state operations manual, Chapter 6 for laboratories. In recent months we have discussed expiration and deletion of some earlier guidance for laboratories and this document summarizes the new expectations in red in the revised SOM. You will want to share this update with your laboratory leadership and learn their perception of actions to be taken.
Nursing Home New/Revised Content Training Materials:
 On January 15, CMS re-released a revised QSO 25-12 for the nursing home industry. This had originally been released November 2024 and discussed in our December newsletter. The revised QSO identifies new or revised content relative to nursing services and analysis of staffing using what they call a payroll-based journal.
On January 15, CMS re-released a revised QSO 25-12 for the nursing home industry. This had originally been released November 2024 and discussed in our December newsletter. The revised QSO identifies new or revised content relative to nursing services and analysis of staffing using what they call a payroll-based journal.
The QSO indicates there are training materials that will be available on their Quality, Safety and Education Portal (QSEP). There is a sign-up process that you will have to go through to access these materials, but there are hundreds of different training materials available. We were not able to find the specific materials related to this QSO, but there is what looks like useful content for all provider types out there.
Consultant Corner

Dear Readers,
If your organization has an internal team for conducting mock surveys and
does not require an external consulting team, our Tracer Team Boot Camp is
the ideal solution to keep your team informed, skilled, and prepared.
This specialized program is designed to strengthen your internal capabilities
by providing:
Exclusive access to live education and training sessions
A comprehensive suite of resources and tools
Hands-on observation of real-time tracer processes
Effective strategies to engage leaders and staff in tracer activities
Empower your team today with the knowledge and skills needed to drive
continuous improvement. Contact us to Train.
Excel. Succeed. Repeat.
Thank You,
Jennifer Cowel, RN MHSA
JenCowel@PattonHC.com
Julia Finken, RN, BSN, MBA, CPHQ
julia.finken@hbsinc.com
Kurt Patton, MS RPh
Kurt@PattonHC.com
John Rosing, MHA
JohnRosing@PattonHC.com