January 2026
Inside This Issue
New Accreditation 360 Survey Process Guide (SPG):

Happy New Year to our readers. By the time you read this JC will already be out there, surveying against their new standards and using their new Survey Process Guide (SPG). The new SPG is probably the most important issue for discussion and the January issue of Perspectives states that JC has already created an updated version of the guide (Dec 2025) that you will want to download and study immediately.
The latest version has gone from 628 pages to 709! Page 2 of the updated version does identify 26 new content items that you will want to study, analyze and evaluate for compliance. These new content issues are underlined to identify them as new in the updated Survey Process Guide. As we have start to learn more and more about their new standards format, we have begun to have a much greater appreciation for the information provided in the SPG. We have previously discussed in this newsletter, and JC’s publications have also discussed the somewhat cryptic nature of the new standards, which figuratively can be condensed to one overarching standard: “comply with law, regulation, NFPA, your policies, your chosen clinical practice guidelines, the CMS state operations manual, and manufacturers instruction for use (MIFU).” However, the SPG provides many, but not all of the details missing from the new standards.

Your author was recently confined on a 5-hour cross county flight and spent the time carefully re-reading the Survey Process Guide, and we believe it contains the key to successfully mastering compliance with the new abridged standards format. In fact, we would encourage our readers to use the SPG exclusively during your preparation and self-evaluation of compliance. Giving a department head a chapter directly from the new standards manual lacks required depth and details that are more easily and better understood by studying the survey process guide.
For 2026, JC has eliminated its “secret surveyor” version of the Survey Process Guide so that healthcare organization leaders can now see the probe questions surveyor will ask, specific documents JC will ask to review, the patients or staff JC suggests the discussion take place with, and the types of compliance evidence JC will be looking for during their evaluation of every CoP. As such, we suggest using the new SPG as an “open book test,” sitting down with staff in different areas of the organization and asking the same questions, of the same staff, and reviewing the same documentation that JC will ask to see. The table of contents section of the SPG is hyperlinked, allowing readers to quickly find their appropriate section, or you could also perform a PDF word search.
Most Frequently Scored, “High Priority” Standards:
We often discuss the most frequently scored standards that are published usually in the Spring each year in Perspectives. The January issue of Perspectives has slightly different approach, discussing frequently scored issues that are also rated as higher risk using their subjective SAFER Matrix. While this methodology doesn’t directly identify the risk of being scored noncompliant on any given standard, it perhaps is indicative of standards that might often be scored noncompliant, leading surveyors to believe there is greater risk, which is a traditional factor in identifying issues that are more likely to be scored at a CoP level.
Another new presentation technique JC uses is that they no longer identify a specific standard or EP, but rather a generic organizational process such as reducing healthcare associated infections, providing a clean and odor free environment, or safely and accurately administering medications. JC has identified five (5) generic clinical areas and five (5) generic physical environment (EC+LS) issues that pose a scoring risk from both a frequency perspective and a clinical risk perspective.
The five generic clinical risk issues are:
- Conducting activities to reduce healthcare associated infections
- Safely and accurately administering medications
- Implementing nursing policies
- Ensuring availability of resuscitation equipment and supplies
- Conducting a pre-anesthesia assessment
The five generic physical environment issues are:
- Maintaining interior spaces that are safe and suitable to the care, treatment and services provided.
- Ensuring critical pressure relationships
- Providing a clean, odor free environment
- Properly handling and storing hazardous chemicals
- Properly maintaining and ensuring safety of furnishings
As you look at these ten (10) generic issues, you may be wondering; “what exactly are they describing.” Well, Perspectives provides some examples of the types of issues that would fall under each generic category. For example, under reducing healthcare associated infections they suggest:
- Expired or improperly stored supplies and equipment
- Noncompliance with infection prevention protocols and MIFU
- Improper use or lack of personal protective equipment (PPE).
We recommend reviewing the entire article and considering your own organization’s risk on these same issues. One issue we wanted to discuss further is the 5th clinical issue about failing to conduct a pre-anesthesia assessment. One of the flaws we have identified as consultants is that anesthesia staff almost always conduct these assessments using standard forms or electronic templates in your EMR. However, at times we do find EMR navigators that struggle to locate this documentation and surveyors may conclude it does not exist.

When non-anesthesia providers administer moderate sedation, which JC considers to be anesthesia, or other forms of anesthesia, these providers may not have a structured form or EMR template that is designed to capture this data. The pre-anesthesia assessment may be embedded in a more comprehensive assessment or form and not easily identified. Unfortunately, it is also sometimes just missing. To the extent you can standardize the approach to documentation among all the specialists who may administer any form of anesthesia, the more likely you are to be able to find pre-anesthesia assessment and evaluate completeness and actual compliance.
 Fire Drills, Water Management, and Above Ceiling Compliance:
Fire Drills, Water Management, and Above Ceiling Compliance:
The January issue of EC News has three (3) informative refresher articles: one on fire drills, a second on water management plans, and a third on compliance above the ceiling. Each is worthwhile reading for those staff involved in managing your compliance in these areas.
In recent months, EC News has had several articles on fire drills, reinforcing the point that the standards for 2026 which in essence requires compliance with NFPA, lack the details that were previously contained in specific elements of performance under EC.02.03.03. After speaking earlier so highly of the new December survey process guide, we looked for the detailed content requirements for fire drills in that document, and we found 20 total references to the term “fire drill” on nine (9) different pages but were unable to locate the specifics about operating room fire drills. EC News reminds readers that OR fire drills remain a JC expectation.
 Hospital Helipad Winter Maintenance and Safety:
Hospital Helipad Winter Maintenance and Safety:
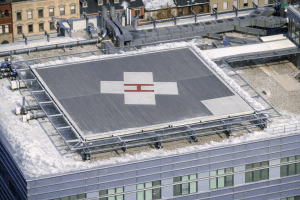
EC News also includes an article on hospital helipad maintenance and winter safety that you won’t find detailed in either the 2025 or 2026 standards manuals. That is because these expectations are from the Federal Aviation Administration or FAA, not CMS. If you have a helipad, do take a look at this article and share with the staff responsible for winter maintenance and clearing the pad. There are specific requirements for how high you can pile snow near the helipad(20 inches high and 20 feet away from the pad, draining away from the helipad) as well as which de-icing chemicals to use (no rock salt or calcium chloride or sand). Do take a look at this article and at how your helipad is maintained.
Case Study: Emergency Planning:
JC published their most recent issue of Emergency Management Leader in the middle of December 2025. The lead article, a case study, highlights some innovative techniques used at the Lehigh Valley Health Network in Pennsylvania, applying their emergency planning to scheduled, community activities such as the annual large crowd NASCAR care race, and an annual employee turkey give away.
 In these scheduled events they get a chance to utilize some of the equipment and techniques that could be implemented in the event of an area disaster. The set up for the employee turkey distribution program looks just like the mass vaccination programs hospitals established during Covid, and they get to practice handling the traffic, logistics, and record keeping. They also discussed a huge portable HVAC system they shared with a community partner during a heat emergency that allowed them to help their community but also practice setting the system up and transporting it to where it was needed.
In these scheduled events they get a chance to utilize some of the equipment and techniques that could be implemented in the event of an area disaster. The set up for the employee turkey distribution program looks just like the mass vaccination programs hospitals established during Covid, and they get to practice handling the traffic, logistics, and record keeping. They also discussed a huge portable HVAC system they shared with a community partner during a heat emergency that allowed them to help their community but also practice setting the system up and transporting it to where it was needed.
We would encourage readers to take a look, not for specific standards compliance details, but rather for some innovative ideas on integrating with community partners and testing concepts out.
EM Planning Templates:
The December issue of EM Leader has an article with multiple links to templates and guidance documents that may help strengthen your EM program. There are many links provided including two links to HVA tools. They include 11 links to EOP templates including specialty areas like psychiatry, rural areas, and home care, seven (7) to continuity of operations planning, five (5) links to communications planning, and four (4) links to disaster recovery. Several of these tools may be useful to your own EM team.
 Disaster Recovery Planning:
Disaster Recovery Planning:
The December EM Leader closes with access to tools for conducting a disaster recovery exercise. There are two links provided to download the tools, one a Word document describing the tabletop exercise and the second a PowerPoint focused on recovery from the disaster. While there is no requirement to utilize these tools, they may prove helpful to your EM team in planning a tabletop exercise.
 DNV Ambulatory Deemed Status Approval:
DNV Ambulatory Deemed Status Approval:
On December 8th, 2025, DNV posted that they had received deemed status approval from CMS for ambulatory surgical facilities. This approval covers a 4-year period from December 2025 through December 8th, 2029.
CIHQ 2026 Manuals and Guides:
CIHQ has posted their 2026 hospital survey process guides and standards to their website where you can download the newest versions. The link to access is found on their Hospitals page.
 ACHC Most Frequently Scored:
ACHC Most Frequently Scored:
In mid-December ACHC published the latest edition of their newsletter called The Surveyor. In this publication they have an article, Hospital Findings Reveal Persistent Compliance Challenges, that details the most frequently scored clinical and physical environment standards for hospitals and critical access hospitals. They also provide advice on strengthening these frequently scored, potential vulnerabilities. Regardless of who you use as an accreditor, we would encourage readers to download this document and analyze your risks in these key problem areas.
ACHC has provided a graph documenting the percentage of hospitals that received findings in these most frequently scored areas. Similar to JC and CMS surveys, infection prevention issues lead the way with approximately 90% of hospitals being scored for these issues. Medication management and nutritional service issues each were scored in approximately 60% of surveys. The frequency of scoring deficiencies in nutritional services was somewhat surprising, however.
The examples provided are known “frequent flyers” on all surveys, but other accreditors might score them against infection prevention or physical environment. Examples of nutritional service deficiencies included food product expiration date management, cardboard storage, direct on the floor storage, spill management, temperature control, dishwasher temperatures, and freezer ice buildup and condensation. Take a look as the issues cited can be problematic in any organization.
Pharmacy Purchasing and Products USP 800:
Last month we summarized some findings from the National Association of Boards of Pharmacy relative to compliance defects identified on surveys that they had conducted on USP Chapter 797. This month we saw an article in Pharmacy Purchasing and Products relative to their annual voluntary survey of hospital pharmacies on USP Chapter 800, hazardous medications. While these are self-reported compliance examples they could pose risk on a survey, or more importantly should an employee develop illness that they attribute to their job duties handling hazardous medications.

The first risk point we noticed was with the development of a hospital’s list of hazardous medications being used. NIOSH did issue a publication last year, but they really have not significantly add new drugs to their list since 2016. Only 19% of hospitals reported that they had personally identified drugs they use that should be considered hazardous beyond what has been on the NIOSH list. This contrasted with 80% of hospitals indicating that they do evaluate the potentially hazardous nature of new drugs they are considering for addition to their formulary. This means the analysis work is being done, but the hospitals list is not being updated to include all the new medications.
A second potential vulnerability noted was that only 44% of hospitals have created a job description for the hazardous drug designated person. More hospital may have identified someone to fulfill this duty, but the detailed expectations and qualifications have not yet been articulated.

Retired Laboratory Memos:
There were no new QSO memos issued this past month, but there were 25 older SC and QSO memos specific to laboratory services that have been officially retired. Some of these memos go back as far as 2009. These older memos became unnecessary as a result of new CLIA regulations being issued back in 2023, in QSO 24-03, which have now become effective.
CONSULTANT CORNER
 Dear Readers,
Dear Readers,
Happy New Year! As we were preparing this issue, The Joint Commission sent an electronic notice to its clients announcing an update to fire drill requirements, noting that the change will be published in Perspectives soon.
🔥 Fire Drill Requirements Update
The Joint Commission has relaxed two long-standing fire drill requirements, eliminating the one-hour minimum interval and the rigid scheduling window. Surveyors have already been instructed to disregard the previous guidance, allowing greater flexibility and a stronger focus on drill quality and life safety outcomes.
Read more to learn what’s changed and how it impacts your compliance planning.
Thank You!
Julia Finken, RN, BSN, MBA, CPHQ, CLSSMBB
Julia.finken@hbsinc.com
Jen Cowel, RN, MHSA
jencowel@pattonhc.com
Yvonne Rockwood, MBA, MHA, CPHQ
yvonnerockwood@hbsinc.com