July 2021
Inside This Issue
Some months there are not a lot of new requirements to discuss, however this month Perspectives announced five sets of new or revised standards. The good news is four of the five don’t become effective until January 2022, and the fifth one that is effective immediately on sprinkler heads is really a simplification of an existing requirement.
The new requirements are in the areas of resuscitation and prevention of workplace violence. The changed standards are in performance improvement and accreditation participation requirements relative to fulfillment of the ORYX performance measurement mandates. Each new or modified set of standards has a brief article and most importantly the link to each of the prepublication standards.
As these will not be available in the printed or E-Edition until later this fall, you will want to make sure each new or changed standards set is downloaded, distributed, analyzed, planned out and ready for implementation on January 1.
 Workplace Violence Standards:
Workplace Violence Standards:
In our view, the most important new standard set in this group, and one that your staff may actually look forward to seeing implementation of, is the prevention of workplace violence standards. These new standards affect three Joint Commission chapters: environment of care, human resources, and leadership.
As you begin your analysis and plan out implementation the first place to start is a very useful portal Joint Commission created specifically on prevention of workplace violence.
It contains a compendium of resources produced by Joint Commission such as their R3 report and a 55-page PDF with many references and links to other resources on workplace violence. There are some questions and answers posed by the industry relative to what TJC means or wants organizations to do for some of the new elements of performance. There are also postings of slides, forms, tools and policies that have been developed by five hospitals around the nation for their workplace violence prevention programs.
After your initial read of the standards, these hospital examples might be the best place to start as seeing innovation and ideas from peers might provide your team a head start on launch of your program.
There is a new element of performance 17 added to EC.02.01.01 which will require an annual worksite analysis related to the organization’s workplace violence prevention program. EC.02.01.01 generally sets expectations for managing safety and security risks, and the new EP 17 establishes a requirement to conduct an annual worksite analysis related to the workplace violence prevention program.
In addition, it establishes a requirement to do something about it, specifically to mitigate or resolve workplace violence safety and security risks based upon your findings from your annual analysis. There is an explanatory note at the bottom of the new EP that helps to define the required annual analysis as a “proactive analysis of the worksite, an investigation of the hospital’s workplace violence incidents, and an analysis of how the program’s policies and procedures, training, education and environmental design reflect best practices and conform to applicable laws and regulations.”
Remember, in a proactive analysis you look to redesign how services are provided in advance of a problem in order to make practices safer, and after you implement changes, you will want to re-evaluate to determine if the changes worked as anticipated and things improved, or you continue to refine the process. There is also an existing EC management plan called the safety and/or security plan which requires an annual evaluation and update of the plan and you will want to incorporate salient points from your workplace violence preventions analysis in that plan too.
There is a minor change to EC.04.01.01, EP 1 which tweaks an existing bullet point on security incidents to state that: the hospital establishes processes for continually monitoring, internally reporting, and investigating “Safety and security incidents involving patients, staff, or others within its facilities, including those related to workplace violence.”
EP 6 of EC.04.01.01 is also modified expanding the current requirement to report and investigate safety and security incidents to now include those related to workplace violence.
HR.01.05.03 is the existing standard that establishes requirements for education and training. Here TJC added a detailed new EP 29 specifically on training for workplace violence prevention. Leaders, staff and licensed independent practitioners will all require training on your workplace prevention program at the time of hire, annually and whenever practices change. The training should include prevention, recognition, response and reporting of workplace violence. We also noted that the training must include de-escalation, nonphysical interventions skills, physical intervention techniques, response to emergency incidents and your reporting process. This is a likely a significant, resource-consuming new requirement for many hospitals.
LD.03.01.01, the existing standard for establishing a culture of safety, has a new EP 9 added to establish a workplace violence prevention program and to appoint a multidisciplinary team and team leader to create the policies and procedures, reporting and analysis of incidents and trends, a follow up process for victims and witnesses, and lastly, a reporting process to the governing body of the organization.
Workplace violence in healthcare certainly isn’t new and many organizations have been tackling this issue prior to these new standards, but this formality requiring a team and leadership involvement, with reporting to the governing body, may help strengthen existing programs and expand the process to organizations that have been slower to develop such an initiative. These standards take effect January 1, 2022 so you will want to think about and develop your implementation timeline and actions to work toward that deadline.

Resuscitation Services Standards:
The next new set of standards we should discuss are the changes to the existing resuscitation standards. The changes affect the Provision of Care Chapter and the Performance Improvement Chapter. PC.02.01.11, EP 1 has an immaterial wording change, but EP 4 is changed more significantly to clarify the expectation for training.
The existing EP described the need for an evidenced based training program, which left many organizations questioning if it meant they had to use the American Heart Association or could they use some other program, and what are surveyors used to seeing? The new EP just describes the need for training, plus it provides guidance that such training should be at orientation, periodically thereafter and when staff responsibilities change.
Note 1 in EP 4 also specifies the training topics should cover “resuscitative procedures or protocols, use of CPR techniques, devices or equipment and the roles and responsibilities of staff during resuscitation.” Note 2 allows the hospital “to determine the format and content of such training, such as a skills day or a mock code.” We should also add that TJC has not softened to the use of any old training program no matter how superficial. The requirement for a sound training program is just moved to PC.02.01.20, below.
There is a new standard created at PC.02.01.20 with three elements of performance. This standard is likely going to require literature search and expert clinical analysis to help with the development of policies, procedures and clinical protocols at your organization. To meet the January 2022 implementation deadline, you will want to start on this standard now.
EP 1 requires the hospital to “develop and follow policies, procedures, or protocols based on scientific literature for interdisciplinary post-cardiac arrest care.” EP 2 also requires the development and adherence to “policies, procedures, or protocols based on scientific literature to determine the neurological prognosis for patients who remain comatose after cardiac arrest.” EP 3 is somewhat similar in nature as it requires “written criteria or a protocol for inter-facility transfer of patients for post-cardiac arrest care, when indicated.”
These three elements of performance are not issues we have previously explored on survey, but we anticipate that many organizations are going to need substantial lead time to identify the appropriate literature, analyze that literature, and reach consensus on policy development.
The existing requirement at PI.01.01.01 to collect data on the results of resuscitation has been changed to add new details on how that data should be collected and what data should be collected. The revised EP 10 now states that the hospital should collect data on:
- “The number and location of cardiac arrests:” Where in the hospital did the arrest occur and how many?
- The outcomes of resuscitation, E.g., return of spontaneous circulation and survival to discharge and transfer to a higher level of care.
There is also a new element of performance 22 added to PI.03.01.01 which requires the development of an interdisciplinary committee to review cases and data to identify and suggest systems improvements in resuscitation. Note 1 provides some examples of some of the issues that hospitals should explore such as missed early “warning signs, timeliness of response, quality of the CPR, post cardiac arrest processes and outcomes following the arrest.”
Some organizations may already have this analysis assigned to a committee, but many others may need to develop such a committee or assign the focus to an existing committee. In terms of your workplan the determination on data collection and post arrest case review can probably be secondary to the development of the policies, procedures and protocols required in the new standard PC.02.01.20.
 Performance Improvement Standards:
Performance Improvement Standards:
The third set of standards changes is in the performance improvement chapter. PI.01.01.01, EP 1 which required leaders to set priorities for performance improvement and to identify the frequency for data collection, has been moved to LD.03.07.01, EP 2. The language about this leadership responsibility is expanded in the number of words used, but the message is essentially the same.
We also encourage our readers to remember that in addition to establishing your own priorities for performance improvement, there are many; what we call “TJC mandatory PI data collection priorities” spelled out in the PI and MS chapters. The previously discussed results of resuscitation and case analysis would be one such example.
PI.02.01.01 has two new EPs, 1 and 2. The new EP 1 adds significant detail to what TJC will be looking for from leaders about their performance improvement priorities. For example, TJC now calls for:
- A written plan
- The defined processes needing improvement including any stakeholder feedback such as patients, staff, regulatory requirements, project goals
- The methods for measuring improvement
- The methods for identifying causes of variation and poor performance
- The methods that will be implemented to address process deficiencies and improve performance
- The methods for monitoring and sustaining the improved process
EP 2 then establishes a requirement to review and update the plan at least annually to reflect changes in priorities in response to changes in the internal or external environment.
There is also a new PI.04.01.01, EP 3 which will require the hospital to use improvement tools or methodologies to improve its performance. Essentially these changes should lead to more structured, formal planning, documentation, improvement strategy, methods and techniques. We anticipate that there will be some necessary work to create this written plan and on survey these changes could lead to some additional findings, so again the advice is to start your modified planning process now in anticipation of 2022.
APR.04.01.01 is the APR that basically requires the organization to submit ORYX performance measurement data to the Joint Commission. They added five new elements of performance and refined another six. The changes almost seem as if they are designed to address a strategy that some hospitals had more than 20 years ago, when the ORYX program was brand new; to select measures that would always be perfect so you would never submit any bad data to Joint Commission. EPs 2, 3, 4, 5 and 20 are new but do not seem to be onerous or create significant new burdens. Basically, these changes require:
- The hospital to select measures that are relevant to the hospital
- Select measures that support strategic measurement goals
- Target high-risk, and problem prone issues
- Provide opportunities to improve the quality of care
- Select new measures if the data are stable and satisfactory
The changed EPs 11, 12, 18, 21, 22, and 24 identify when you should change measures and when you may not change your measures, and when you must submit the measure data. While the number of changes to this APR may look significant, it should not be if you are measuring performance in meaningful areas that are intended to help your organization improve care. The one issue you may need to review carefully is if you had plans to switch measures, to verify that this is permissible under the new APR.

Spare Sprinkler Heads:
The fifth change discussed in Perspectives this month is in the life safety code chapter and specifically the requirement for spare sprinkler heads. Not too long ago, TJC had changed LS.02.01.35, EP 7 to require organizations to store six spare sprinkler heads of each type and temperature rating that the hospital uses. When that change was announced it appeared controversial and potentially costly and laborious as many organizations have lots of sprinkler heads and types.
Well, the change announced in the July issue of Perspectives removes the word “each” and simply states you must have at least six spare heads that correspond to the types and temperature rating of the ones in use. This expectation of at least six spares is if you have 300 or fewer sprinklers and the total number of spares goes up proportionately in accordance with NFPA 13-2010. That would be a minimum of 12 spare heads if you have up to 1000 sprinklers and 24 spares if you have greater than 1000 sprinklers.
We assume that TJC and CMS are on the same wavelength on this change, however, additional reading, blogs, and web postings we have seen indicate that this may still be subject to continued discussion as interpretation of AHJ’s or authorities having jurisdiction may have differing opinions. We advise our readers to be on the lookout for any additional or different interpretations or guidance they see from others. But for now, this appears to be a simplification of an existing requirement.
 eProcessing Bloody Surface/External Ultrasound Transducers:
eProcessing Bloody Surface/External Ultrasound Transducers:
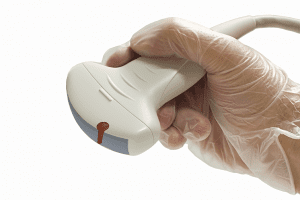
This month’s Consistent Interpretation column discusses an important issue that we as consultants have been discussing among ourselves and with clients and that is how to process surface, external ultrasound transducers that come in contact with blood or body fluids.
The format of the Consistent Interpretation column is not ideal for drawing conclusions because you hav surveyor observations and canned guidance that may or may not directly address the surveyor’s issue. However, there are three conclusions we can draw from this month’s column.
The first, which has become somewhat of a TJC mantra, is that reprocessing guidance should be developed based on the transducer manufacturer’s instructions for use, or MIFU. Second is that reprocessing guidance should be based on the intended use of the transducer and this relates back to the Spaulding classification system of critical, used in body cavities and requires sterilization, semi-critical, which comes in contact with mucus membranes and requires high level disinfection and noncritical, which comes in contact with intact skin and requires low or intermediate level disinfection. The third issue is on the use of a sheath and its impact on reprocessing requirements.
This blog is an explanatory narrative format and it states some important information regarding the use of a sheath:
- The FDA has stated the use of a sheath on a transducer does not change the Spaulding Classification of the transducer, as these sheaths may leak or tear. Therefore, it does not change the minimum level of reprocessing required for the transducer based on clinical use, unless otherwise indicated by the manufacturer. As the MIFU have to be approved by the FDA, it would have to be a validated device and sheath combination to alter the standard reprocessing advice.
- If the intended use of the transducer and the usual Spaulding guidance do not align with the MIFU guidance you must contact the manufacturer to ensure you can perform effective reprocessing for that intended use. For example, if the transducer normally only comes in contact with intact skin and is cleaned by performing low level disinfection, but your intended use will bring it in contact with blood or body fluids, and the MIFU is silent on such use, then contact the manufacturer for guidance.
We would also advise that if you are faced with the second scenario above and you have to contact the manufacturer for guidance to try and obtain written guidance, or keep detailed, contemporaneous notes about who you spoke with and what guidance was provided. The issue we see most often on consultative surveys is a surface transducer being used during a procedure that will bring it in contact with blood or body fluids. We sometimes hear from clients that they use a sterile sheath and therefore do not think they need to perform high level disinfection. Such responses are going to need additional documentation from the transducer and sheath manufacturer going forward.
 Emergency Coordinators:
Emergency Coordinators:
Earlier our discussion about Perspectives had a lot of important “to-dos” in preparation for new standards that will be subject to survey in 2022. This month’s EC News has a several highly informative articles that may help make your programs better, but there are no time sensitive deadlines approaching to make these happen. The lead article in EC News is about designating an effective Emergency Coordinator.
Two very useful pearls are identified through weblinks to online and in person training programs and two different potential certification options for your emergency management lead. Too often the EM lead is one more job duty on someone’s already full plate. The training and certification opportunities that are available to someone on your team might help create an advancement opportunity for that individual and more importantly help develop a better emergency management process at your organization. The article is worth sharing with your team and considering use of the training or certification programs.
 Extreme Temperature Preparation:
Extreme Temperature Preparation:
The second thought provoking article is on preparation for temperature extremes. Extreme heat or extreme cold can be a disaster scenario if electric or HVAC goes out during a weather emergency and the risk for such an emergency is one that should be considered on your hazard vulnerability analysis.
This article provides a nice mitigation and preparedness checklist of questions to help organizations self-assess their readiness for such extremes.
 Crash Carts:
Crash Carts:
The third article we wanted to draw your attention to is “What’s your Question, What’s your Solution,” this month discussing best practices and common findings relative to crash carts. One such issue they discuss is, does TJC expect crash carts and defibrillators to be plugged into emergency powered outlets? TJC states here that it is not mandatory, however they would expect the organization to have a process in place to keep equipment charged during a prolonged power outage. One issue they did not mention that we have seen TJC advise previously is to conduct a risk assessment to determine if you can choose not to plug into emergency powered outlets. This may help you think through the advantages and disadvantages of using emergency powered outlets.
The article reminds readers that crash carts that are in departments that are not open 24/7 should be locked in a secure location during off duty hours. The authors also restate from a 2017 Quick Safety the most common types of survey findings relative to crash carts that are seen on survey. The article mentions the most common finding we see which is a failure to check the crash cart per the schedule required. We would add to that list in EC News that in recent years we see common findings for open and undated EKG electrode packets, and defibrillator checking procedures that are not consistent with the device MIFU.
 COVID-19 Data:
COVID-19 Data:
The last four months we provided the link to the data CMS is analyzing relative to Covid-19 test positivity in counties throughout the US. CMS and Joint Commission have been examining this data to determine suitability for survey. We have reproduced that link again for your use: https://data.cms.gov/stories/s/q5r5-gjyu.
2/24/21 3/23/21 4/27/21 5/28/21 6/22/21
Green 1327 Green 1892 Green 1795 Green 2286 Green 2707
Yellow 1541 Yellow 1154 Yellow 1209 Yellow 826 Yellow 505
Red 337 Red 113 Red 204 Red 44 Red 20
As you can see the number of green counties with less than 5% test positivity rate continues to grow. The yellow counties with 5-10% test positivity and the red counties with greater than 10% continues to diminish. All of which means we are moving in the right direction.
 Emergency Management Exercise Waiver:
Emergency Management Exercise Waiver:
On June 21, 2021 CMS reissued last year’s QSO-20-41 which had discussed waiving the next full emergency management exercise for organizations that had activated their EM plan and evaluated their response. At this point many organizations have deactivated their EM plans, while some others are still active. CMS wanted to clarify who gets waived, what they get waived from, and what year’s exercise they are waiving. We should also mention that this modified memo requires a careful read.
The nature of the waiver is not as wide open as some of the language might have you believe. The waiver only applies to the full-scale exercise, not the “exercise of choice.” If an inpatient facility is still operating in 2021 under its emergency plan, CMS states “it will be recognized by surveyors as having met the full-scale exercise requirement for 2021 (even if it claimed the exemption for the 2020 full scale exercise).”
Remember, however, that CMS has added an element of complexity to the schedule by application of its 12-month expectation. They expect completion of EM exercises on a 12-month schedule, not anytime within a year. So, if you continued with your EM plan as activated until May of 2021, at which point you deactivated your EM plan, and your full-scale exercise was due sometime prior to May 2021, you are exempt. However, if your next full-scale exercise was not due until November 2021, you will still have to conduct that full scale exercise as planned. Read through this QSO memo carefully before deciding to waive your annual exercise to verify that you really qualify for waving that exercise.
Emerging Infectious Disease Preparedness:
The Inspector General published a report in June 2021 discussing CMS’ controls related to hospital preparedness for an emerging infectious disease. You don’t have to do anything as a result of this report, but it is an interesting read and to some extent might help predict things to come in the future. Their conclusion is that CMS had a well-designed process, but they need more control over accrediting bodies. Specifically, it mentions that CMS issued regulations in February 2019 which required hospitals to add the issue of emerging infectious disease to their emergency management plan.
Since the memo was issued in February, after many organizations might have updated their plans for 2019, CMS anticipated that all others would update at the start of 2020. Unfortunately, early in 2020 the pandemic hit (an emerging infectious disease) and accrediting bodies largely stopped surveying. Thus, CMS was not sure that every accredited hospital had updated their EM plan appropriately, even though you were actively managing an emerging infectious disease at the time.
The document indicates CMS conducted “targeted infection control surveys” at hospitals that don’t have deemed status through an accreditor, and at those who do have deemed status, but had deemed status suspended as a result of CMS finding serious deficiencies during a complaint survey. The IG report indicates that accreditors did not perform comparable, targeted infection control surveys.
So, while you may have been relieved those accreditors were not performing surveys and you could focus your energies on patient care, apparently the OIG is suggesting that was the wrong approach for the accreditors to have taken. We also noted that while CMS provided comment in the IG report, none of the accreditors did, but they may offer feedback in their own defense soon on their websites.
Consultant Corner
Dear Readers,
Just as a reminder, we do not publish in August, so we will be back in September!
Have a wonderful rest of your summer!
Jennifer Cowel, RN MHSA
JenCowel@PattonHC.com
Kurt Patton, MS RPh
Kurt@PattonHC.com
John Rosing, MHA
JohnRosing@PattonHC.com
Mary Cesare-Murphy, PhD
MCM@PattonHC.com